
In healthcare, knowledge has an expiry date. Scientific evidence, digital tools, biomaterials, pharmaceuticals, and clinical guidelines all evolve so rapidly that what was standard practice a few years ago can quickly become outdated.
Alas, medical education in Nepal struggles to keep up with this pace of change. The number of medical, nursing and dental schools in the country has surged in the past three decades, but instruction and training remains poor and largely uneven.
Curricula often take years to change, faculty development varies widely between institutions, and many educators have limited access to or knowledge of the latest scientific advances.
The bigger problem begins once students graduate. They leave medical school believing that a degree marks the end of formal learning rather than the beginning of a career of continuous education. That is not a personal failing as much as a systemic one. Our education system still treats a medical degree like it is a one-time vaccine providing lifelong protection.
It is tempting to argue that reforming this will take time, and that better governance will eventually solve this problem. But medicine cannot wait for bureaucracy. Every year that medical education falls behind, patients receive care that may already be obsolete.
LIFELONG LEARNING
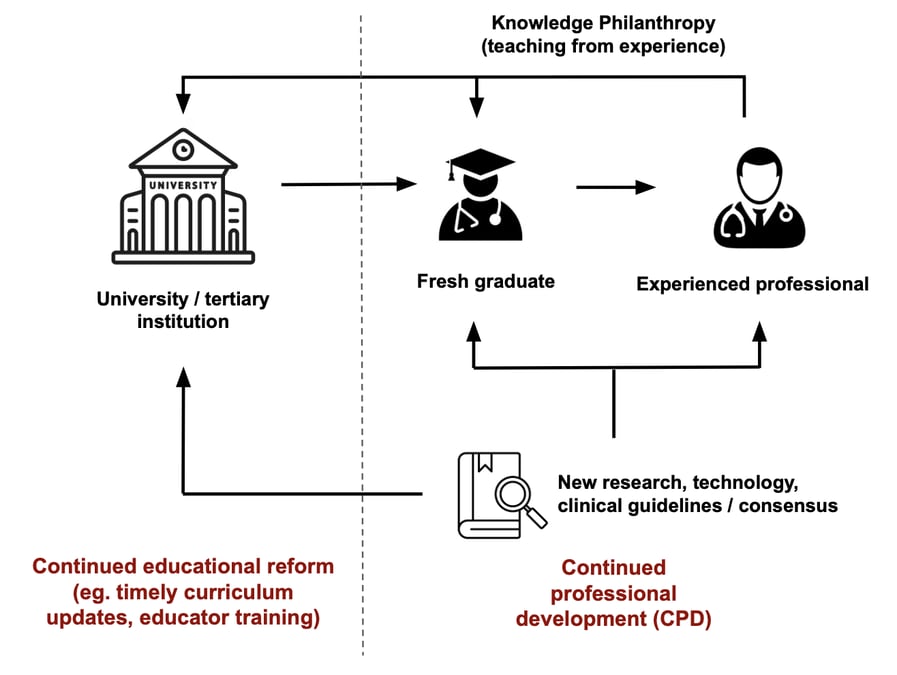
This is where continued professional development (CPD) becomes indispensable. While universities and medical schools work to modernise undergraduate and postgraduate education, CPD ensures that practicing healthcare professionals are not left behind.
It transforms learning into a lifelong professional responsibility through accredited courses, conferences, workshops, self-directed learning, and peer collaboration. Clinicians can keep pace with evolving evidence, emerging technologies, and continually changing standards of care.
Around the world, CPD systems differ in how they are funded and delivered, but the strongest ones share the common principle that lifelong learning is a professional responsibility rather than a personal choice.
Nepal has been laying the regulatory foundations for such a system. The Nepal Nursing Council now requires nurses and midwives to complete 60 CPD credits over six years, with at least 10 credits earned annually, for license renewal.
The Nepal Medical Council has also introduced a framework requiring doctors to complete 100 CPD credits every five years, although this has yet to be enforced as a mandatory requisite for license renewal.
Yet, mandating credits is the easy part, creating high-quality learning opportunities across the country is far more difficult. This demands coordination between employers, professional associations, regulators and government to identify national learning priorities, accredit educational activities, assure quality, and evaluate whether CPD is actually improving clinical practice and patient outcomes.
Without such coordination, CPD risks becoming a box-ticking exercise in which credits are accumulated but competence remains unchanged. Many CPD systems in low and middle income countries have struggled because of inadequate funding, limited technological infrastructure, insufficient administrative capacity, and the absence of robust strategies to address the shortage of training resources in rural regions.
No amount of regulation or infrastructure can, by itself, create a culture of lifelong learning. Policies may require clinicians to participate in CPD, but they cannot compel intellectual curiosity or professional generosity.
Ultimately, the success of any CPD system depends on two commitments: healthcare professionals who remain willing to learn throughout their careers, and experienced practitioners who are equally willing to teach what they have learned.
Every experienced healthcare worker possesses a body of practical wisdom that cannot be fully captured in textbooks or clinical guidelines. It is accumulated through years of recognising subtle clinical patterns, managing complications, learning from mistakes, and refining judgement in situations where evidence alone offers no clear answer.
When this knowledge is not shared, each new generation of clinicians is forced to rediscover lessons that their predecessors have already learned, while decades of expertise disappear each time an experienced practitioner retires or leaves the workforce.
This is where the idea of knowledge philanthropy becomes essential. Nepalis often associate philanthropy with donating money or material goods, yet the sharing of knowledge can be equally transformative. Mentoring junior colleagues, delivering lectures, leading workshops, facilitating case discussions, publishing educational resources, or hosting webinars all multiply the impact of a clinician's experience far beyond the patients they treat directly.
Such knowledge transmission does not replace the need for systemic reform, but it provides the cultural foundation that allows CPD to evolve from a regulatory obligation into a shared professional ethic.
Technology has made this easier. Recorded lectures, virtual case discussions, digital libraries, and interactive learning platforms have largely removed the geographical barriers that once limited continuing education. What remains is the will to recognise that teaching is an integral part of professional responsibility.
For a successful, home-grown culture of life-long learning to take root in Nepal’s healthcare, here are four action points:
Hospitals integrate teaching into daily clinical practice. Clinicians who mentor juniors, lead case discussions, conduct journal clubs, or develop educational materials are granted protected teaching time. These contributions are formally recognised in appraisals, promotions, and leadership appointments.
Universities transform into lifelong learning hubs. Medical, nursing, and dental schools appoint experienced clinicians not only as visiting faculty but as professors of practice. These experts help incorporate more practical and time-relevant teaching methods into the curriculum and strengthen partnerships with hospitals and professional associations, ensuring education aligns with modern clinical realities.
Professional councils evolve beyond mere credit tracking to reward knowledge philanthropy by delivering accredited lectures, mentoring juniors, publishing educational materials, and facilitating workshops.
Senior healthcare professionals share knowledge as a core clinical and ethical responsibility.
A CPD system driven by knowledge philanthropy is the most practical, sustainable, and culturally resonant way for Nepal to ensure that its healthcare professionals remain competent, and its patients receive the best possible care.
The question is no longer whether we can afford to invest in this movement but whether we can afford not to.
Sushil Koirala is a practicing dentist and former president of the Nepal Dental Association.