

Nepal’s oxygen emergency has eased somewhat as the Covid-19 second wave crests, but the crisis exposed serious gaps in the supply and distribution of medical oxygen with major implications for the future.
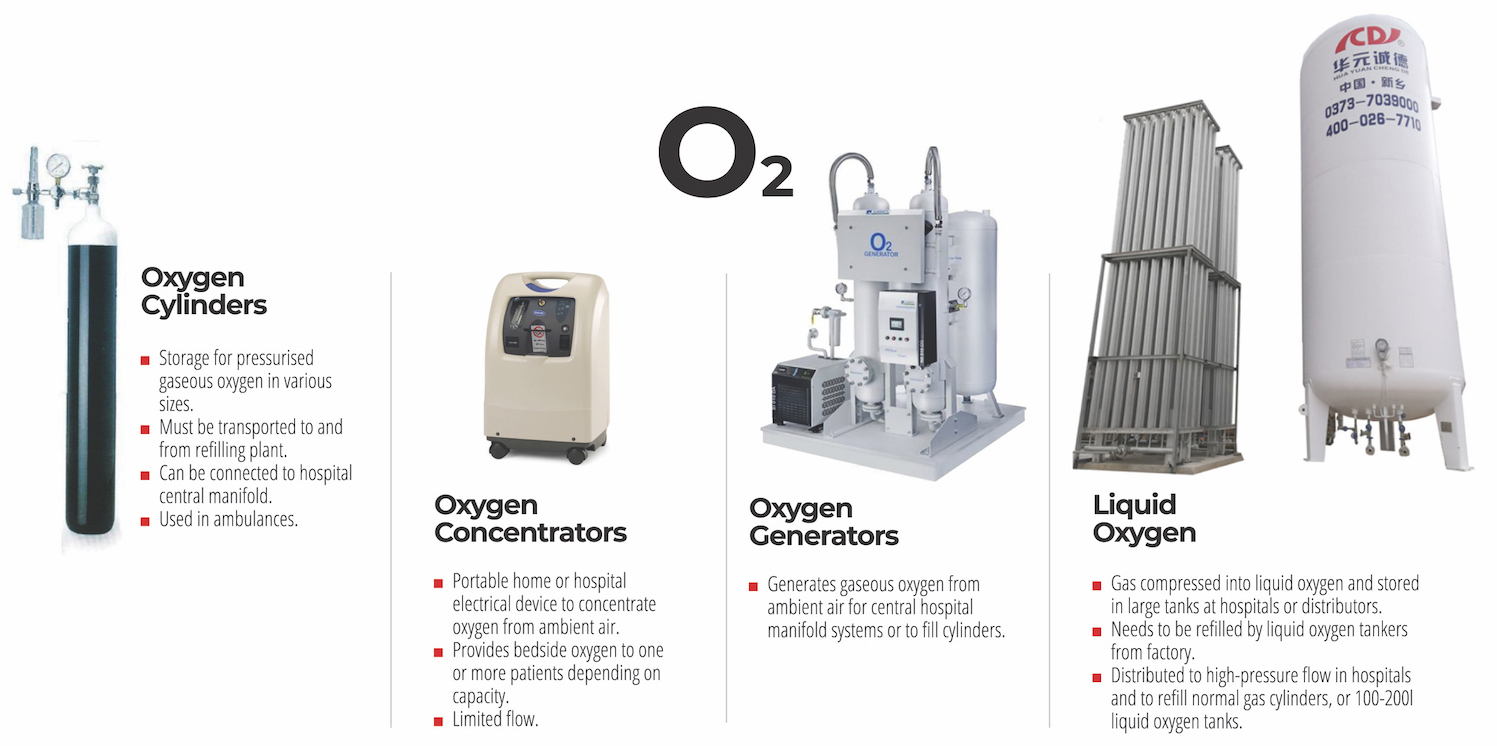
At the peak of the second wave, many Covid-19 patients died as hospitals ran out of oxygen, but with an overwhelming international response to rush cylinders, concentrators and generators, there is now the risk of over-capacity of medical oxygen post-pandemic.
Nepal’s demand for oxygen cylinders shot up to 50,000 per day during the peak of the second wave in May, with the country’s oxygen factories and hospitals only able to fill 19,000 cylinders every day. In contrast, pre-wave calculations had suggested that peak daily demand would only be about 6,000 cylinders.
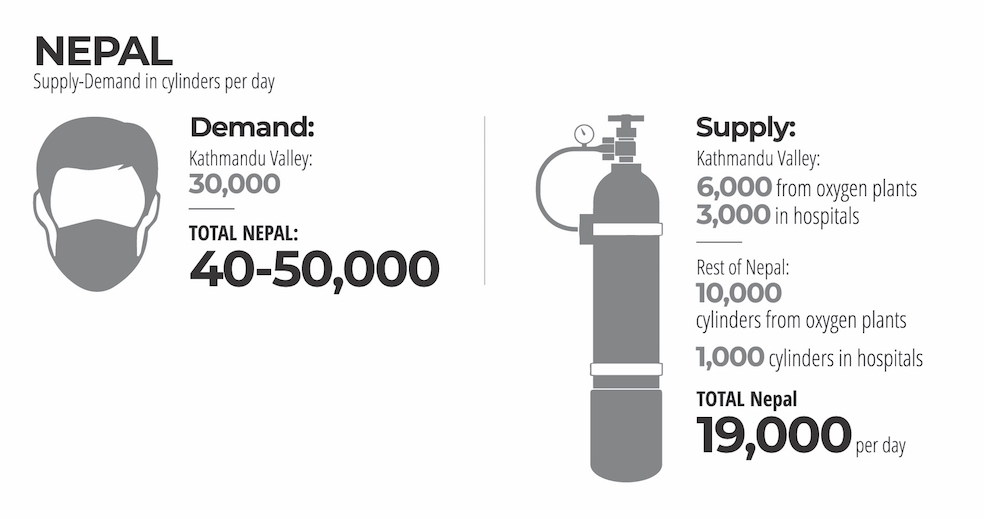
Most of the 29 oxygen factories in Nepal were working at only half capacity pre-pandemic because of low demand. In fact, three of them had closed down. As the second wave hit, the plants went into full-scale production, but a shortage of cylinders meant that the excess production could not be sent to hospitals.
Meanwhile, factories relying on liquid oxygen tankers were affected by an Indian ban on export. Empty cylinders from China, Oman and other countries alleviated the shortage somewhat, while oxygen plants grappled with increasing generation capacity.

Too little too late
When the inter-ministerial Covid-19 Crisis Management Center (CCMC) finally reacted, it was too late. Its arbitrary quota system for every hospital proved disastrous.
“The quota resulted in hard-hit hospitals being undersupplied and safer hospitals being unnecessarily saturated with cylinders,” explains Roop Jyoti, former chairman of Grande City Hospital, suggesting the problems lay in supply chain management rather than oxygen production.
Faced with mounting criticism for bungling the oxygen quotas, the Health Ministry resorted to micromanaging, and ordered suppliers to only send filled cylinders to hospitals that had its recommendation letter.
The result was catastrophic, many hospitals were either forced to refuse service or they asked families of patients to bring their own full cylinders.
In a notice posted in mid-May, Kathmandu’s Om Hospital said: ‘Under the capping made by the government on oxygen supply, we are unable to take admissions despite our willingness to provide service. We have enough manpower such as doctors and nurses to take care of patients but not enough oxygen supply.’
Families with Covid-19 patients hoarded full cylinders at home, and desperate ones rushed to the gates of oxygen factories to buy the life-saving gas. Municipalities, especially in areas with spare capacity, prevented the transport of oxygen beyond district borders.
Most of Nepal’s oxygen plants are in central and eastern Nepal. The Morang-Sunsari industrial corridor alone had five large oxygen factories with surplus capacity, but these were prevented from sending supplies to hospitals in Kathmandu and other areas with shortages.
Lack of training in oxygen flow management and ventilator use did not help matters. Makeshift local isolation centres with non-medical staff were using full flow to treat patients with mild symptoms. Hoarding and black marketing was rampant, and while large hospitals ran out of oxygen supply, local isolation centres had one cylinder per patient.
In Grande International Hospital, there was a 30% drop in oxygen demand when doctors were more judicious in oxygen use. Still, the shortage was serious enough for some doctors to ration oxygen even for their most serious patients. Others had to make the difficult choice between continuing to put patients who had little chance of survival on oxygen, or to give it to those who would immediately recover with oxygen.
Even before the pandemic, government oversight on cylinders was non-existent with no standardisation or regulation in place regarding colour coding, pressure, price rates and deposits on oxygen cylinders.
“I used to get desperate calls at 3am from families of patients desperate for oxygen. We were able to call up spare capacity during the second wave, especially in the east of the country, but the shortage of cylinders for refilling did create a temporary shortage,” says Gaurav Sharda of the Nepal Oxygen Industries Association (NOIA).

After the peak
With the first week of June, Nepal’s Covid-19 curve started flattening with hospitals in Kathmandu and major cities seeing fewer patients who needed to be on oxygen or in ICU.
“Compared to the devastating shortages in April and May, oxygen availability is relatively stable,” says Anup Bastola, a physician at Teku Hospital. The Ministry of Health also seems to have learnt from its mistakes, and is ensuring a more equitable supply of cylinders. Donated oxygen concentrators are now being flown to district hospitals where they are needed.
However, even as demand for oxygen goes down, overseas Nepalis and international donors are still rushing empty cylinders, concentrators, generators and liquid oxygen tanks on relief flights to Kathmandu. There are more oxygen generator plants arriving from France, the US and China this week. Ventilators from international donors are sitting idle at some district hospitals in western Nepal because no one knows how to operate them.
Domestic oxygen production itself is now reaching 100% capacity. Even though there is a challenge of logistics, equitable distribution, and cost, Nepal will soon have more oxygen than it needs. What the government needs to focus on is getting much-needed oxygen to rural areas where the virus is spreading house-to-house.
The flood of donated oxygen generators now means that there will be domestic over-capacity just as there was before the second wave. Nepal’s oxygen sector therefore needs to balance supply to meet demand surges and periods of low consumption.
Explains Jyoti: “Ironically, many new donated oxygen plants are being set up in hospitals in response to the second wave, so when this passes, there will be tremendous over-capacity. Regular factories would probably have to function at less than 25% capacity and will be destroyed financially.”
At Teku Hospital, Bastola says repurposing oxygen equipment could help Nepal prepare for future spikes. If there is a third wave this autumn, for example, demand would go up again. Besides Covid-19, there is also the pre-existing need for oxygen to treat the rise in respiratory ailments such as COPD and heart disease caused by worsening air pollution.
Says Sharda at NOIA: “One of two scenarios can now play out. The government could either continue its reliance on donated oxygen generation equipment, thereby driving Nepali producers out of existence, or it could encourage sustained domestic production to meet a spike in demand during future outbreaks.”
Last month, reports of Pressure Swing Adsorption (PSA) oxygen plants failing in hospitals, and a CCMC finding of 70% oxygen leakage in many hospitals were overlooked. These issues are structural and if resolved can help alleviate future shortages.
“The government’s approach to oxygen distribution was myopic,” says Sharda. “Oxygen is a basic product and can easily be bottled here. But they failed to consult with us producers, and now all this oversupply from abroad will jeopardise our ability to respond to future outbreaks. Plant staff should also be treated as frontline workers and have vaccinations.”
The government and CCMC failed to acknowledge that assistance was needed in the oxygen supply chain rather than production, and by allowing import of production equipment but bungling on supply management, they failed to take into account domestic generation capacity, thus increasing vulnerability in the future.
The only solution to prevent another oxygen crisis is to stop the problem at the source, by stemming the spread of Covid-19. But the lesson from the second wave is that Nepal’s government, hospitals and oxygen plants need to have standby capacity at hand for future waves.