

Turn off the hectic East-West Highway at Chandrauta, bump up a short dirt road, and you reach the equally busy Basic Health Services Hospital in Shivraj Municipality, Kapilvastu District. Small groups of people gather around its two single-storey buildings — some line up, others fan themselves in the morning heat.
To the left is a new, smaller building. The main room is unfinished and boxes of supplies are scattered on the floor, but other areas are being used. At one end, a pharmacist sits at a window serving a line of people outside. In an office at the other end, a nurse at a desk talks to a pregnant woman during a pre-delivery (antenatal care, or ANC) visit.
“This Smart Integrated Clinic will be a one-stop shop for mother and child healthcare,” says Hospital Director Birendra Kumar Mishra. Financed by the municipality and equipped by UNICEF, the clinic will focus on vaccinating children in the hospital’s catchment area of nearly 100,000 people.
To date only about 70% of kids in the area get vaccinated due to low awareness or hesitation among locals, or because many born at the hospital are from families who live elsewhere.
“Many families from outside can’t afford to wait until the next vaccination day; the Smart Clinic will offer inoculations daily so they won’t have to,” says Mishra, sitting in his office with the ceiling fan whirring. Its records will be linked to a Government of Nepal information system, so if a mother or child misses an appointment they can be traced and contacted, he adds.
In an email, UNICEF credits proactive local leaders and a strong willingness to invest in innovation for the Smart Clinic, which is soon supposed to start delivering other services like nutritional counselling by female community health volunteers (FCHVs).
But like much of maternal and newborn health (MNH) in Kapilvastu, in Lumbini Province, and across Nepal, news at the Basic Hospital is not all positive.
About a month later in the same office, Dr Amit Pandey is explaining the recent death of a pregnant woman. Close to her delivery date, she arrived at the hospital with high blood pressure (known as pre-eclampsia) and severe anaemia.
Doctors referred her to the provincial hospital in Butwal, but her family took her home instead. Eight days later she returned, unconscious. Again, doctors referred her to Butwal but the family again returned home.
The next day she hadn’t improved so the family decided to follow the doctors’ advice but the woman, a mother of three, died on the way to the facility. “They are very poor,” said Pandey. “We referred the case but they didn’t want to go to a higher centre — they were worried about the cost. We even offered them a free ambulance but they didn’t take it.”
Ironically, two days earlier the Director of the Lumbini Province Health Directorate singled out the referral system as a weakness in the province’s healthcare.
“Our referral mechanisms are very poor,” said Roshan Lal Chaudhary in an interview in Taulihawa. “For example, we lack facilities in Kapilvastu, so from Kapilvastu Hospital a referral would be made to Butwal. We prepare the papers, but they don’t go. Sometimes it’s a financial issue. It could also be because they lack confidence speaking or they don’t know anyone there.”
Asked if Lumbini Province will meet the 2030 target for maternal mortality in the United Nations Sustainable Development Goals (SDGs), “it will be difficult,” said Chaudhary.
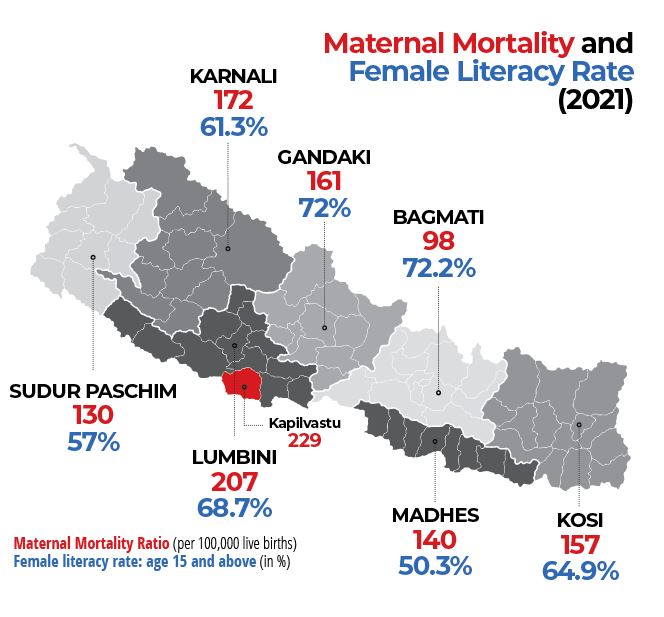
The Report on Maternal Mortality, part of the 2021 census, put Nepal’s maternal mortality ratio (MMR) at 151 deaths per 100,000 live births. Lumbini was the highest among provinces: 207 (see map). Kapilvastu’s MMR was 229.
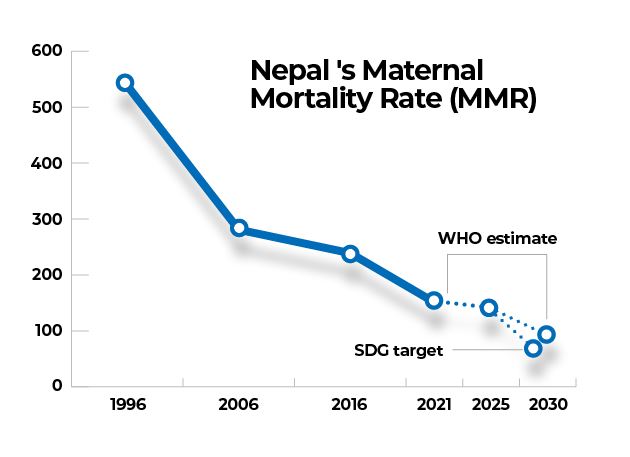
In February 2025, the World Health Organization (WHO) estimated the national MMR had dipped to 142. Between 2016 and 2023 it fell 5.8% yearly, added the report. If that trend is maintained, WHO predicts that Nepal’s MMR will reach 93 by 2030, missing the SDG target of 70.
Early triumph
In 1996, Nepal’s MMR was 539 but by 2016 it had dropped to 239 and the country was celebrated globally for reducing maternal deaths. While progress has slowed, multiple efforts are being made by Nepal’s health community, including all three levels of government, to regain momentum to meet the SDGs target.
But inadequate funding from the central government and the sudden cut earlier this year of millions of dollars injected annually by USAID have made that climb steeper.
Kapilvastu followed the national trend — it made a huge improvement and then momentum braked. Home deliveries, which are riskier because they usually occur without skilled medical staff, dropped from 2,256 in 2019-20 to 284 in 2024-25, according to local non-government organisation (NGO) Kalika Self-Reliance Social Centre.
But with larger marginalised communities, whose members are less educated and more conservative, and frequent movement across the border with India, the challenge in Kapilvastu is greater. For example, between 2020-21 and 2022-23 the number of deliveries attended by a skilled birth attendant fell from 60% to 54%, according to the health directorate’s annual report. Births in health facilities dipped from 60% to 58% in the same period.
Lack of awareness seems to be on the lips of everyone asked to explain Kapilvastu’s maternal and child health issues. At Ganeshpur health post in Bijaynagar Rural Municipality, in-charge Gautam Roy is hoping that replacing 10 of 12 FCHVs, who retired, will spark greater awareness-raising but he says the scope for gain is limited by the community.
“We have fewer home deliveries now—just one or two a month compared to five when I arrived five years ago—but some local people are not well educated so they don’t follow our advice,” says Roy, sitting behind the desk in his office.
“They don’t make a plan, so when a woman has to go for delivery they don’t call the transport on time. In other cases, they don’t know the date of delivery, even though the health post calls them regularly to remind them,” he adds.
The situation varies from municipality to municipality and even from ward to ward. In Buddhabhumi Municipality, six wards had zero home deliveries in the previous year, the other four will reach the target this year, says Mayor Keshav Shrestha. One of those wards is Muslim majority, he adds, sitting on a couch facing a steady stream of service seekers coming through the office door.
Now in his second term in office, Shrestha says it’s clear why his government is investing in maternal and child health: “If we don’t look after these basic needs, then the community will not be developed for the future.”
Marginalised communities
The Madheshi and Muslim communities are often singled out for avoiding healthcare services. “In those communities the literacy rate is a little lower and the decision-making power of women is less,” said Chaudhary.
For example, Muslim women are the least likely group in Nepal to deliver in a health facility (67%); most common are Brahmin/Chhetri women (87%), found the 2022 Nepal Demographic Health Survey.
Muslims make up 18% of Kapilvastu’s people.
At the Basic Hospital, director Mishra says Muslims don’t necessarily lack awareness — some community members believe that their religion bars the use of certain services.
The INGO Fairmed has worked on MNH in Kapilvastu since 2011. Country Coordinator Nirmala Sharma says her team worked directly with Muslim religious leaders. “We developed a trust with them… those who got sensitized went to their mosques and sensitized people. Still, they can’t guarantee that 100% of people will comply.”
Teacher Niyaz Ahmad says that he has been encouraging family planning within the Muslim community since 2016. “I tell them, ‘planning starts before marriage. You have to choose your wife, your partner for life. After that, when do you want to have a child’?” he says in an interview at a local madrasa.
“After your first child, you must wait a minimum of two years to have your second. Otherwise, your child could have health problems, your wife could have health problems. It could be three years, four years — it depends on your wife’s health, your baby’s health.
The point is not to limit family size but to plan, says the teacher, founder of Madrasa Jamia Matalul Uloom Alsalafia, in Mayadevi Rural Municipality. “You can have one child, or three, or two but you have to make a plan.”
“These ideas are found in Islam, in the Quran, in the Prophet’s sayings,” adds Ahmad, who works within a programme known as Khusahal Pariwar, managed by the UN Population Fund (UNFPA) via a local NGO.
In Shivraj Municipality the use of family planning has risen 45% in the past 4 years, says UNFPA. Maternal and child health statistics have also improved, says the agency. For example, the number of women making four ANC visits rose 66% and facility deliveries jumped 101%.
Khushal Pariwar concepts have also been included in the class 8 health education curriculum and endorsed by the Madrasa Board of Lumbini Province and the National Madrasa Association, says the UN agency.
Auxiliary Nurse Midwife Anjali Sahani says she has seen a change in the behaviour of Muslim women using the Bardahawa basic health service centre in Kapilvastu Municipality ward 2. “Today they come the same as other pregnant women come for their checkups and have home visits after delivery.”
Matron Leela Sharma says she has seen awareness grow among women in general during the seven years she's worked at Kapilvastu Hospital. More of them are going for more ANCs — the protocol recently increased from four to eight visits.
Demand is also rising for family planning and gynaecological services. “Maternal mortality today does not happen much at home but on the way to the hospital,” Sharma adds in an interview at the hospital.
The 2021 census report found that 57% of maternal deaths occur in facilities, 26% at home, and 17% on the way to a facility.
That report sparked a renewed focus on quality of care. “Women want to come to health institutions, but are they properly taken care of? This is the major challenge,” says Mahesh Maskey, Executive Chief of the Nepal Public Health Foundation, whose team just finished collecting and analyzing 15 months’ data on maternal and newborn deaths in Kapilvastu.
To boost quality of care nationwide, the family welfare division (FWD) of the department of health services (DoHS) bought dozens of anti-shock garments for remote facilities, to treat women who haemorrhage following delivery. The suits stabilize their condition until they can be moved to a better-equipped facility.
Post-partum haemorrhage is a leading cause of maternal death worldwide and was responsible for 26% of maternal deaths in 2021, found the census.
Labs survive USAID cut
In Kathmandu, the National Health Training Centre worked with WHO and other partners to develop a training module to enhance the skills of nurses working in MNH.
The pilot session was delivered in April at the new Maternal and Neonatal Simulation Lab Centre of Excellence in the new building of the Paropakar Maternity and Women’s Hospital.
The centre was conceived as the first of seven labs in hospitals across Nepal where MNH workers could practise their existing skills and learn new ones, using advanced mannequins.
The project lost its funding when USAID stopped running in early 2025, but the implementing partner, One Heart Worldwide, is raising money to replace the $1 million-plus budget, says Co-CEO Surya Bhatta.
“We are still finalizing the revised timeline, but our goal is to complete these labs within the next two years,” he says in an interview.
Asked if Nepal’s USAID funding could be fully replaced, Bhatta says, “OHW has always been a diverse pool of funders, so we were able to cope with the situation and are hoping that this will continue, but the future is going to be very challenging as there will be a lot of competition for the resources.”
Other MNH initiatives cut after the departure of USAID include a suite of items to boost breastfeeding rates across the country: hiring of 36 nurses trained to work in 18 hospitals in all provinces, equipment for the country’s only milk bank, at Paropakar Hospital, and the opening of UNICEF-sponsored lactation management units in eight hospitals across Nepal.
Health Minister Pradip Paudel did manage to get a small increase in the health budget for the current fiscal year. Some of it will be used to hire public health officers to work in every municipality across Nepal, a move that Bhatta says, “if implemented well, could significantly strengthen our preventive, promotional, and basic health care systems, including MNH.”
The FWD also announced in June that lost USAID funding for a key micronutrient survey will be replaced by another US agency.
Still, Paudel recently told a ministerial meeting in Geneva that foreign aid cuts put Nepal’s MNH progress at risk. “Vital services for nearly five million women and nutrition programmes for 1.5 million children under five have been affected,” said the minister, as reported by the Kathmandu Post.
Despite Chaudhary’s negative forecast, maternal deaths plummeted in Lumbini in 2024-25, from 82 the previous year to 57, according to the health directorate’s annual report. Other positive signs: the percentage of pregnant women having eight ANCs rose from 28% the previous year to 58%; the percentage having four postnatal checkups climbed by 21%, to 56%.
But the picture painted by the latest DoHS annual report is, surprisingly, darker. Key statistics nationwide have declined in the previous year. Facility deliveries fell by 5%, deliveries by specially trained staff declined by 6%, and the rate of women getting four ANCs dropped by nearly 6%.

Every mother counts—so count them
When the 2021 census found that Lumbini had the highest maternal mortality ratio (MMR) of the 7 provinces (207 deaths per 100,000 live births), “it was very surprising,” says Mahesh Maskey, Executive Chief of the Nepal Public Health Foundation (NPHF).
After analysis, the NPHF team and partners decided that if they could increase the annual drop in the MMR to 25% from the trend of 6-7% a year, they could reach the SDGs target of 70. Other provinces would follow suit. They chose to focus on Kapilvastu because the district had been well studied but still had one of the highest MMRs in the province (229).
“Reaching 25% seems very difficult but if you think of it, if there are four deaths in one place the first year, you only have to reduce that by one to have a 25% reduction the next year,” says Maskey during a presentation at the NPHF office.
“With close supervision, monitoring, and all the facilities that government is providing for maternal health, it is doable. Provincial and local governments are highly committed. Lumbini Province has allotted Rs126 million for MNH this fiscal year and municipalities have committed to reduce maternal mortality to zero,” he added.
First, NPHF needed an accurate picture of pregnancies in the district. Over 15 months, the team collected data on every pregnant woman in 8 out of 10 municipalities.
“Once we have the data, each and every mother should be followed up — are they prepared for the birth, where do they want to go for delivery, do they have complications, what are health staff advising?” says Maskey.
Data analysis can reveal significant trends, but is not being done now, he added. For example, is there a correlation between the average age of new mothers and the health of women and their children?
The data showed that the MMR in the municipalities varied widely. The lowest had zero deaths over 15 months; the highest MMR was 695. Interestingly, the local unit with the highest MMR was in the mid-range for home deliveries - 9%. (The lowest was 2%, the highest 16%).
NPHF presented the results to policy makers in the province and nationally. “They agreed that our main focus has to be quality of care — how to strengthen the hospital, the centre; how to encourage them, motivate them,” says Maskey. “The more the clinical centres become attractive for delivery, the more people will give up home delivery and go there.”
Politics before newborns
Prior to Covid-19, the INGO Fairmed agreed to a request from the then chief of the Kapilvastu Hospital in Taulihawa and invested Rs1.5 million to build a special newborn care unit (SNCU). It opened in June 2018 and ran until the hospital paediatrician left a couple of years ago, each month serving 15-20 newborns with severe illnesses.
The paediatrician wasn’t the only specialist who left. The exodus happened after the hospital chief, a political appointee, was moved out following a change in government and replaced by a junior doctor, who many of the seniors didn’t want to work under, according to a media report.
Earlier this year a new hospital head was appointed but as of press time he has yet to take up his duties, and no money has been included in the current year’s budget to run the SNCU. That means families with seriously ill newborns must travel to larger centres for care, like Lumbini Provincial Hospital in Butwal.
“It’s so sad,” says Fairmed Country Coordinator Nirmala Sharma. “That’s one of the hospitals we invested a lot in. We had to renovate the building, buy and install the equipment — the director was very happy.”
One-quarter (24%) of all cases nationwide admitted for specialized newborn care in 2023-24 came from Lumbini, according to the DHS annual report.
The director of the Lumbini Province Health Directorate, Roshan Lal Chaudhary, says there is nothing he can do. “We have no influence on this — it’s a political issue.” In fact, the hospital in Piuthan district is facing the same situation, he adds.
The writer made two trips to Kapilvastu. For the first, Fairmed provided local transportation and logistics support. For the second, UNFPA provided a flight ticket plus local transportation and logistics support. Editorial control remained with the writer and Nepali Times.