

On a late afternoon in August 2022, Sushila Bohara, 19 and nine months pregnant, started complaining of a sore stomach. Soon after, she went into labour. Within 30 minutes she had delivered a baby girl outside of her isolated village home in Rukum West district, but her abdominal pain only got worse. About a half hour later she died.
Over a year later details of the young woman’s death at her husband’s family home in Todke village, Chaurjahari Municipality were unclear, even after interviews with her mother-in-law, a sister-in-law, staff at the local health post and the chief of the municipal health department.
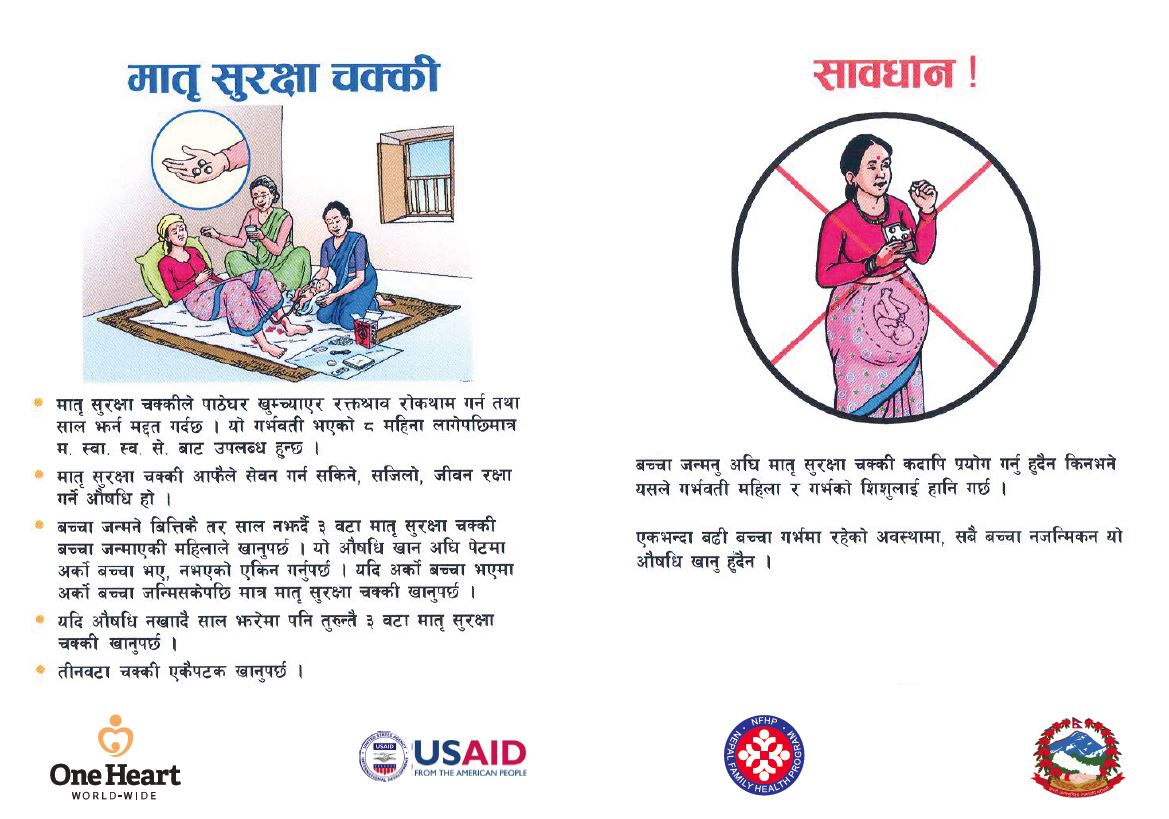
But one thing seems certain: Sushila did not receive the matri surakshya chakki (MSC) that is supposed to be given to every pregnant woman in Nepal who is at risk of having a baby without a health worker attending.
The MSC packet of three pills of the drug misoprostol is meant to be given in advance and can be taken by women immediately after they deliver their baby, to prevent excessive bleeding. Also known as post-partum haemorrhage, or PPH, such bleeding is the number one direct cause of maternal deaths in Nepal.
World Health Organisation (WHO) guidelines, from 2020, recommend advance misoprostol distribution to pregnant women for prevention of PPH.
Nepal’s 2021 census reported 622 maternal deaths; 162 (26%) of them happened at home.
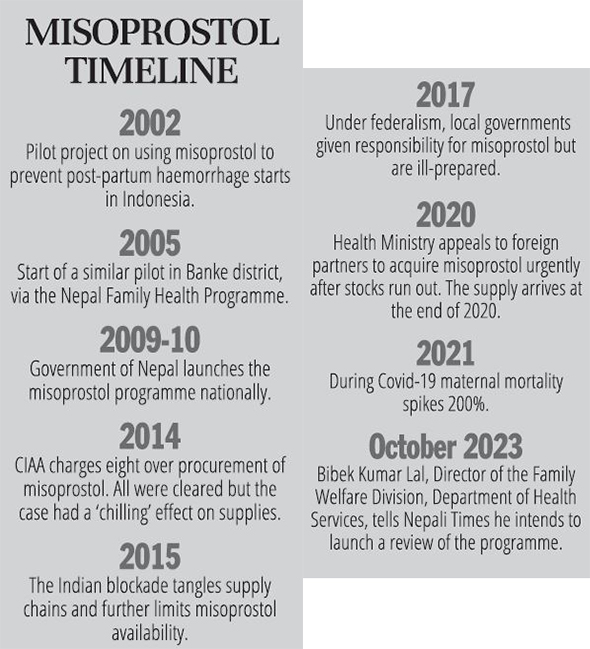
In October 2023, Bibek Kumar Lal, director of the family welfare division (FWD) of Nepal’s department of health services (DHS), told Nepali Times he would initiate a review of the programme after hearing the story of Sushila Bohara.
Since early 2000s
In interviews, public health workers recalled the effort it took in the early 2000s to convince officials in the ministry of health and population and the WHO to agree that providing misoprostol was the right way to improve Nepal’s deadly maternal mortality ratio. At the time, it was 281 deaths per 100,000 live births a year. Today it is 151, while the target set for 2030 in the Sustainable Development Goals is 70 or less.
A main reason for official reluctance was a misplaced belief that giving the pills to pregnant women in their 8th month (in case their baby came early) would encourage them to deliver at home instead of going to safer health facilities.
Nearly two decades later that argument is still heard in maternal health circles in Nepal. Combined with a series of unrelated events that interrupted the rollout of misoprostol across the public health system, it has led to some of the most at-risk women in the country dying needlessly.
Bali to Banke
Misoprostol was actually developed in the 1980s as a drug to treat ulcers. But in 2002 a pilot project was launched in Indonesia to see if misoprostol could help to prevent PPH, in part because unlike other medicines, such as oxytocin, it didn’t need to be refrigerated or injected, making it well suited to poorer countries. PPH then caused about half of Indonesia’s 18,000 maternal deaths yearly.
The study found that women who used misoprostol were about 25% less likely than other women to perceive excessive bleeding after birth, 30% less likely to need emergency care for a birth complication, and 45% less likely to need emergency care for PPH. News of the pilot’s success soon reached Nepal, where PPH was also a leading cause of maternal deaths.
In a 2021 interview Ashoke Shrestha recalled a visit by one of the researchers who worked on the Indonesia project. “He did a presentation on the latest evidence on different interventions to reduce PPH and he just had this little inkling of an idea based on partial data from Indonesia. We all sat there and said ‘Aha!’.
“The idea took a while to mature and grow on us,” added Shrestha, who was then deputy chief of party in Nepal for John Snow Inc (JSI), one of the international health organisations collaborating in the Nepal Family Health Programme (NFHP). NFHP was launched in 2002 and funded by the US Agency for International Development.
“We worked on the paperwork to pilot an intervention… we had a fairly good set-up in Banke and we kind of embedded this initiative into the ongoing community-based maternal and newborn programme,” recalled Shrestha.
Then director of the family welfare division (FWD), Yasho Vardhan Pradhan, remembered that before the pilot programme launched, maternal mortality “had become a very serious concern.”
“We had a negligible number of skilled birth attendants, or trained health workers. There were few health facilities that could provide normal delivery facilities and if there were any complications… they had to refer to higher facilities, which were next to impossible to access,” Pradhan added in a 2021 Zoom interview.
When the misoprostol roll out was proposed, “there were reservations from our professional organisations, mainly from the national association of obstetricians and gynaecologists,” he remembered. “They were a little bit reluctant to delegate authority to community health volunteers, they were concerned of the possible complications and consequences.”
Shrestha recalled facing “a lot of resistance from the medical profession. Their logic was that as a general policy the government was trying to promote institutional delivery. This (misoprostol) plan would compete with that objective.” But advocates of the initiative reassured opponents that, “the gold standard is that you deliver at an institution but (misoprostol) was plan B,” said Shrestha.
Some officials at WHO headquarters in Geneva were also reluctant, recalled Stephen Hodgins, then chief of party for JSI. They were OK with misoprostol being used at home births but only if directly administered by a health worker.
Nepali officials were also divided about permitting rural women to themselves take the drug, recalled Hodgins, now an associate professor in the School of Public Health at the University of Alberta in Canada, who still advises on health projects in Nepal.
Because of the scrutiny of the plan, “it was very important for us to show that women complied with instructions, so we had very close monitoring,” added Hodgins over Zoom in 2021.
Lifesaving project is born
Nepal’s misoprostol pilot project occurred in the rural areas of Banke district, and was seen as important enough to be inaugurated by the minister of health.
Starting in 2005, it included training female community health volunteers (FCHVs) and other health workers to: identify the pregnant women in their area, provide pre-birth health education, dispense misoprostol (three tablets of 200 mg) in the 8th month, and make home visits soon after delivery.
A review by the NFHP found that ‘among the 11,658 women reached with misoprostol over the first 18 months of the program (about 73% of all the women pregnant in rural Banke) there were only 16 deaths, i.e. fewer than half the expected number (33).’
A 2010 study led by obstetrician Swaraj Rajbhandari, who worked on the pilot project, noted that of about 840 women who filled out surveys 73.2% said they received misoprostol, while others took oxytocin. Both drugs help to prevent PPH by causing the uterus to contract.
Overall, the proportion of births that included one of the two drugs meant to prevent dangerous bleeding rose from the expected 11.6% to 74.2%. ‘Those experiencing the largest gains were the poor, the illiterate, and those living in remote areas,’ the study found.
The review also noted a larger increase in facility deliveries in Banke over two years than in the rest of the country, which was chalked up to an overall rise in counselling to pregnant women via the NFHP.
In a recent interview Rajbhandari said the results reinforced the belief that oxytocin alone was insufficient to meet the risks posed by home deliveries, mainly because it requires cold storage and must be injected while misoprostol can be stored at room temperature and swallowed.
According to Pradhan, “after piloting everyone, even professional organisations, senior consultants, gynaecologists and obstetricians, they all agreed that the programme should be expanded to those places where health facilities and trained health workers were not available.”

Sushila Bohora’s home
It is a 10-minute downhill scramble along a barely visible path to reach Sushila Bohara’s home in Chaurjahari Municipality, hidden behind a screen of short, leafy trees. Nimble white goats and brown chickens forage around the worn path that surrounds the small, single-storey stone building.
Two hours earlier we had left Kotjahari town behind, smoothly winding uphill in our jeep, the view of the valley and river below slowly expanding as we rose, before lurching off the pavement to rumble and bounce to the end of the narrow road.
Sushila lived here with her mother-in-law and sister-in-law while her husband worked in India, the two women explain perched atop an underground water tank, metres away from the house.
“She lived here for about three years. She was quiet and good, which is why God took her,” says mother-in-law Deuma Budathoki, wistfully, as tears grow in her eyes.
Yamuna Budhathoki cradles her son in her lap as the two explain how Sushila died, five days before her due date. “She started complaining of a sore stomach around 4PM and gave birth about a half hour later. She was happy and healthy at that time.
“But soon after, she said her stomach was hurting again. She asked for hot water, and drank some, but it didn’t help. A half hour later she died.”
The women say that when Sushila’s pain didn’t diminish her brother-in-law ran to a local private medical clinic to get a stretcher. Soon, she was writhing in distress in Yamuna’s arms. Sushila died about 5PM, one hour after going into labour.
The family called a doctor from a private clinic, who came and pronounced her dead, but didn’t give a cause of death. Days later two FCHVs visited with an official from the municipality’s health office. Their report says that Sushila died of PPH.
Growing pains
When the misoprostol programme was taken over by the Government of Nepal in 2009-10 it had spread to at least 14 districts, according to the DHS annual report.
But while the initiative appeared to be thriving, sustainability did not seem to be a priority. Shortages or ‘stockouts’ became routine. JSI’s Shrestha remembered the government having to request an emergency procurement from a global partner in the years following its takeover of the programme.
Those shortages might have motivated one director-general to order excessively when supply finally became available, triggering a corruption investigation, Shrestha added.
It appears too that the rollout of the programme into a new district was most effective on paper. Some — but not all — FCHVs appear to have been trained. And they were provided with MSC but only if it was in stock.
‘Many of the FCHVs were not supervised and of those who were supervised 42% were not asked about progress relating to misoprostol,’ found a 2014 evaluation of the programme, done by a team that included Rajbhandari.
The review said that FCHVs assumed that as more birthing centres opened, women would use the facilities to give birth. As a result, ‘a great proportion of FCHVs do not keep stock of misoprostol with them nor do they distribute to pregnant women. Because of this, women delivering at home without the help of a health worker are at higher risk of PPH.’
Only 13% of women who gave birth at home in that period received the tablets, reported the 2016 Nepal Demographic and Health Survey.
Interviewed recently, Rajbhandari said the evaluation showed clearly that FCHVs were getting mixed messages about misoprostol. “One was ‘take them to a health facility, don’t let them deliver at home’. I fully encourage that, as an obstetrician. Everyone should be delivering in a big hospital if possible so that all complications can be managed.”
“But what if they deliver on the way or at home? For those women, we do need some kind of alternative medicine to prevent PPH.”
After the evaluation the government committed to look into the problems. “I think it improved slightly,” remembers Rajbhandari.
But a 2017 assessment sounded a cautionary note: ‘In Nepal, women who receive advance misoprostol are both willing and able to use the medication for PPH prevention during home births. However, the supply and personnel challenges identified raise questions about scalability and impact of the program over the long-term.’
Lifesaver or barrier?
Despite a series of phone calls en route to arrange an interview, Sushil Pokhrel is not to be found when we reach Rukum West District Hospital in Musikot. An orthopaedic surgeon, Pokhrel is medical superintendent of the government hospital and head of the district’s Health Services Office.
When he finally strides up the hill in a half-sleeve shirt and sits at a table outside of the canteen, you feel it’s for minutes only, until another phone call pulls him away.
Very soon Pokhrel is echoing many people who have opposed the misoprostol programme since it began in 2005. “This should not be the practice. On one hand you are encouraging institutional delivery, on the other hand you are giving misoprostol to FCHVs. What that says is that you are empowering FCHVs to deliver babies and promoting home delivery, not institutional delivery.”
In exceptional cases misoprostol can be used, adds Pokhrel. “But we are in the 21st century — we can do things like station an ambulance close to health facilities, track patients using mobile apps, instruct FCHVs to inform us when complications appear and we can have a team ready to respond.”
In Kathmandu, the offices of the FWD are found in a gloomy building in the department of health services compound at the end of a short, bustling alley in Teku. Director Bibek Kumar Lal sits alertly behind the desk in his large office, offering seats to a guest and three members of his staff.

Lal says the misoprostol programme is misunderstood, in part because the government hasn’t explained it well.
“It was never meant to replace institutional deliveries. Sometimes people would argue that by raising awareness about this misoprostol programme we are somehow telling the pregnant woman and her family that it’s fine to deliver at home because once you take these tablets you’d be safe, but that was never the intention of this programme.”
Adds the director, “you see more and more deliveries happening at health facilities, so the misoprostol usage has gone down. But I also accept that there are still pockets where we have an unacceptably high level of out of health facility delivery and the programme still focuses on those districts.”
He adds, “Misoprostol still has a very important role to play in those situations where we see the woman delivering at home and dying from excessive bleeding which could easily have been prevented by providing these simple pills. So the programme has not lost its relevance.”
Obstetrician Rajbhandari argues that both misoprostol and oxytocin are still needed in the fight against PPH because it remains the top direct cause of maternal death both at home and in health facilities. Along with FCHVs, health staff in facilities should also be trained to distribute MSC, she adds.
“The good news is that oxytocin is available in 94% of facilities, although the quality is not consistent,” said the doctor in an interview at a clinic in Lalitpur. As for misoprostol, “even in the Tarai I would say that it has to be available in the smaller pockets where women do not go to hospital, and in the Himalayan and hilly areas definitely.”
Officially the misoprostol programme today operates fully in 56 districts and in 14 others staff have been trained but MSC hasn’t been distributed.
The number of women who took misoprostol decreased in the three years preceding the 2022 annual report of the department of health services, from 10,874 to 8,613, to 7,496. That dovetails with the rise in births in facilities, which went from 64% in 2016 to 79% in 2002, according to the 2022 Nepal Demographic and Health Survey.
The 2021 census put the maternal mortality ratio at 151. Fifty-seven percent of those deaths happened in facilities, 26% at home and 17% on the way to a health facility. It did not say how many women who died at home had used misoprostol.
Alleged corruption
With weaknesses already starting to show in the supply and distribution of misoprostol, in 2014 the programme was rocked by an investigation by the Commission for the Investigation of Abuse of Authority (CIAA). Eight health department officials were charged for allegedly importing faulty misoprostol at inflated prices.
All were eventually acquitted by the special court but the incident appears to have had a ‘chilling’ effect.
After the CIAA case, recalled former director-general Pradhan, “procurement was not done for two or three fiscal years, there was a shortage of misoprostol. Because if you were to start a procurement process you’d think that you’d be watched by the CIAA, so everybody was afraid of procurement.”
In 2021, Leela Khanal, remembered a big supply gap after the investigation was launched. “The new director sent a letter to all the international partners to supply the product, and they did, but it was not sufficient to cover all districts,” said Khanal, who later became JSI’s chief of party in Nepal.
The devastating earthquake of 2015, followed by the unofficial blockade by India, further worsened misoprostol procurement by tangling supply chains.
Though it had expanded on paper to 48 districts when Nepal switched to a federal system in 2017, the misoprostol programme already appeared shaky. Under the new governance set-up, responsibility for the drug, and other maternal and child health medicines, was passed to local governments.
Many of them had no idea what misoprostol, or MSC, was, says Surya Bhatta, executive director of the international health organisation One Heart Worldwide (OHW), which has worked on maternal and child health in remote areas of Nepal for 13 years.
“It’s not like building a road in your town… you really need to have the technical capacity to understand why this is important,” Bhatta said in a 2021 interview.
Some local governments didn’t act, resulting in shortages, with potentially long-term consequences, said Bhatta. “Once (the supply chain) is broken, women’s behaviour will change. They will forget about the programme… if they get the medicine after two years they will not accept it.”
Just before the Covid-19 outbreak in 2020 the shortage became critical. While the misoprostol programme had expanded to 58 districts on paper, cupboards in health facilities were empty. In April 2020, according to Punya Poudel, chief of FWD’s safe motherhood unit, only 16 of 77 districts across the country had a supply of misoprostol.
In June 2020 government officials called international partners to a meeting and asked for help. UNFPA and OHW responded with emergency supplies months later.
Disconnected
The roof of the Chaurjahari Municipality office building in Kotjahari town is a great place to enjoy the sun and the view of surrounding hills and valleys. Visible northward across the curving Bheri River is the cluster of hillside buildings that make up Khalanga, the main centre of neighbouring Jajarkot district.
Closer and veering east is Purtimkanda, with a health post of the same name, less than an hour’s walk from Sushila Bohara’s house. Staff at the health post say that Sushila visited the day before she died, and was healthy according to their tests and observations.
The health post had a supply of misoprostol around the time that Sushila died, says the municipality’s health coordinator Ram Bahadur Sunar sitting behind the desk in his office a couple of floors below. “We don’t know if the health post in-charge is giving it to the FCHVs, but we are providing it.”
Sushila’s family says the woman didn’t receive misoprostol and was not visited by an FCHV during her entire pregnancy, because the volunteer was based in Kotjahari at the time, too far for regular visits.
Officially the misoprostol programme was launched in Rukum in 2012-13, the district split into Rukum East and Rukum West post-federalism in 2017. OHW began its programme in the district in 2023.
Over six years it will help the district to build needed infrastructure, such as birthing centres, train health service providers and FCHVs, and help stakeholders improve services, says Lok Mani Giri, OHW district coordinator.
He says his team gave ‘refresher’ training on misoprostol to all of the district’s relevant health personnel in 2023, and at least 50% were unfamiliar with the drug and the government programme when the course began.
One observer in Rukum West told Nepali Times that if OHW hadn’t launched the training, the misoprostol programme would still be stalled in the district.
Sunar says that ending home births is the number one priority of his office, and Sushila’s death is, above all, the result of an unfortunate lack of communication, adds Sunar. “A mother losing her life is definitely a tragedy… Our commitment is that no mother should be in such a situation.
“When she was delivering, the family called a private clinic, they didn’t call the health post, so we couldn’t do anything,” adds the official. “There are many birthing centres within people’s access but they don’t inform us about coming births — that’s why we are so sad about this case.”
In Surkhet the provincial government’s top health official also points to a breakdown in communications for the flaws in the misoprostol programme.
“Before federalism there was one chain of command, starting with the federal government going down to the community,” says Rabin Khadka, director of the health services directorate, in an interview in his office. “Nowadays it’s not like that — each level of government has its own system.”
“From the provincial side we only provide technical support to them and the programme was actually launched from the federal government. But the implementing agency is the local government, and monitoring and support should be done by them,” adds Khadka.
While health access has improved overall under federalism, the misoprostol programme has its shortcomings, Khadka added. “Most of the local health facilities we visited have a misoprostol programme but some of them didn’t have stock, because there was a shortage.”
“Other facilities have thrown away their stock of misoprostol because they didn’t know what it was — the staff was new. But in our overall system we have a sufficient amount of misoprostol.”
In Kathmandu, Lal echoes his provincial colleague: “With federalisation the three tiers of health services got disconnected and the gap between them is gradually expanding. Without any chain of command there is no means to ensure accountability of the programme as well as to verify the reliability of the programme being conducted in any one district or municipality.”
“The majority, perhaps, of the responsibility falls on our shoulders,” Lal continued. “I do not shy away from that. But as I told you, we are responsible for providing budgets… now the basic health services are maintained at the municipal level. It is the districts who are supposed to procure and supply the medicines.”
According to Bhatta of OHW, “we know that the programme should be working much better than what is happening right now… that’s the main reason why we are also making an effort to deliver this misoprostol training programme to health workers and FCHVs.”
“At the policy level we have the right policy, we have a system,” he adds. “In the implementation we need to really focus… The municipality, local health facilities, and probably the federal and provincial governments can reinforce one another, do review and planning together.”
“Maybe in 10 years or 15 years home delivery will be zero,” added Bhatta, “then we might roll back the misoprostol programme, but today this emergency drug is still needed.”
How to explain why a project designed to meet such an obvious, urgent need, which launched with so much promise, has kind of stuttered and stumbled over the years? Could that be because misoprostol targets some of the most marginalised people in Nepal: rural women who lack access to health facilities?
Nepal’s constitution says that ‘every citizen shall have the right to free basic health services from the state, and no one shall be deprived of emergency health services.’ But Lal acknowledges that “those who at the margins are the ones who are always left out, in most of the programmes.”
“In Nepal we have several programmes with incentives added in, particularly for those women and children who for financial hardship cannot even afford to come to health facilities… but still they are left out… It’s not about now passively serving them — we need to be more active and reach out to them.”
“There are multiple issues that need to be looked into,” concludes the director, “and I think it’s high time that we did a comprehensive study, which would provide us objective information on why the misoprostol programme is not working — we don’t even know the level at which it is functional at the moment.”
Asked if such a study is realistic Lal says that he will need to find external funding for it but that it is “absolutely realistic”.
Corruption probe slowed programme’s rollout
After a lifetime working in Nepal’s health system Mingmar Gyalzen Sherpa knows that change happens slowly. “In my village in Solukhumbhu it took 10 years just to teach them that every pregnant woman has to be examined by a health worker. That is all I wanted to teach.”
“They would say ‘my grandmother delivered three kids at home no problem, why shouldn’t I’?” said Sherpa in an interview in Surkhet district in October 2023.
It’s ironic then that the doctor was at the centre of a court case that seems to have delayed the nation-wide rollout of a lifesaving programme for pregnant women.
In 2014, he and seven others linked to the procurement of misoprostol, a drug used to prevent excessive bleeding in mothers who have just given birth at home, were charged by the Centre for the Investigation of Abuse of Authority (CIAA). They were accused of buying too much medicine at inflated prices.
Sherpa and the others were acquitted by the special court after a probe, but the doctor said he is still waiting for the Supreme Court to clear his case.
“It did some damage to the programme,” recalled Yarsho Vardhan Pradhan, who was director-general of the department of health services directly before Sherpa occupied the chair.
“The procurement issue definitely demoralised all health workers and the motivation to expand and to continue misoprostol intervention became seen as somewhat fishy, even development partners starting thinking ‘oh, this has started happening—people are making money’.”
“I don’t think it was a case of an individual person getting greedy,” said Ashoke Shrestha, who worked with JSI, one of the international health organisations that collaborated to introduce misoprostol in a pilot project in Banke district in the mid-2000s.
“The fact that he was acquitted seems to imply that he was above the law when he did the procurement.”
Seizing an opportunity
Shrestha recalled that Sherpa had simply taken a good opportunity. “They hadn’t been able to procure (the drug) in the preceding one or two years – there were shortages… when you have that ‘famine’ and you see an opportunity – you go for it.”
Sherpa had retired as director-general by the time of the investigation. He believes now that his frank manner offended an international partner, which provoked a complaint to the corruption authority.
“The CIAA called me up and said, ‘Some organisation called and said they are not happy with you. What happened? You used to be a nice person.’ I said ‘I’m still a nice person, I haven’t done anything wrong. But if someone does something and I’m not happy, I say plainly that I’m not happy.’ And many people don’t like that.”
Today, Sherpa, who was bestowed the Madan Bhandari National Award for 2079 for his work in medical science, is dedicated to embedding mobile ultrasound machines in the health systems of Nepal’s rural areas to monitor the health of pregnant women.
He spent three years training nurses in Far West province how to use the machines, and is now teaching others based in Karnali province.
After completing a three-week course combining theory and practice, each cohort of 20 nurses goes home with a battery-operated ultrasound unit. “Almost all complications can be detected with the help of an ultrasound,” said Sherpa.
These include twin pregnancies or babies in a breach position in the womb, conditions that can’t be handled at a health post and after detection will be referred to larger facilities.
“Before being trained, nurses would send every case to the doctor, after this training the doctors will come and ask them, because doctors themselves (except radiologists) are not trained on how to use the ultrasound,” he added.
Reporting for this story was supported by Medecins Sans Frontieres (MSF)/Doctors Without Borders as part of the Without Borders Media Fellowship. One Heart Worldwide provided logistics support.