

As the school year drew to a close in April, kindergarten teacher Sharmila Gurung, 27, was summoned to the principal’s office and was told to resign because her English-language instruction was ‘inadequate’.
But her ouster had nothing to do with English proficiency, it was her HIV status. She was also told to transfer her 7-year-old daughter to another school.
“That’s when I realised they somehow found out that I was HIV positive,” recalls Gurung. “I felt numb and couldn’t speak for myself.”
Her teaching job in Kathmandu paid just Rs13,000 a month, and half of that went towards rent. As a single mother, she is now worried about her daughter’s education.
This was not the first time Gurung has been stigmatised over her HIV status. Four years ago, she was fired from a Montessori school in Gorkha after the staff learnt of her diagnosis and parents threatened to withdraw their children from school. She resigned and moved to Kathmandu, but ostracisation due to ignorance and stigma pursued her.
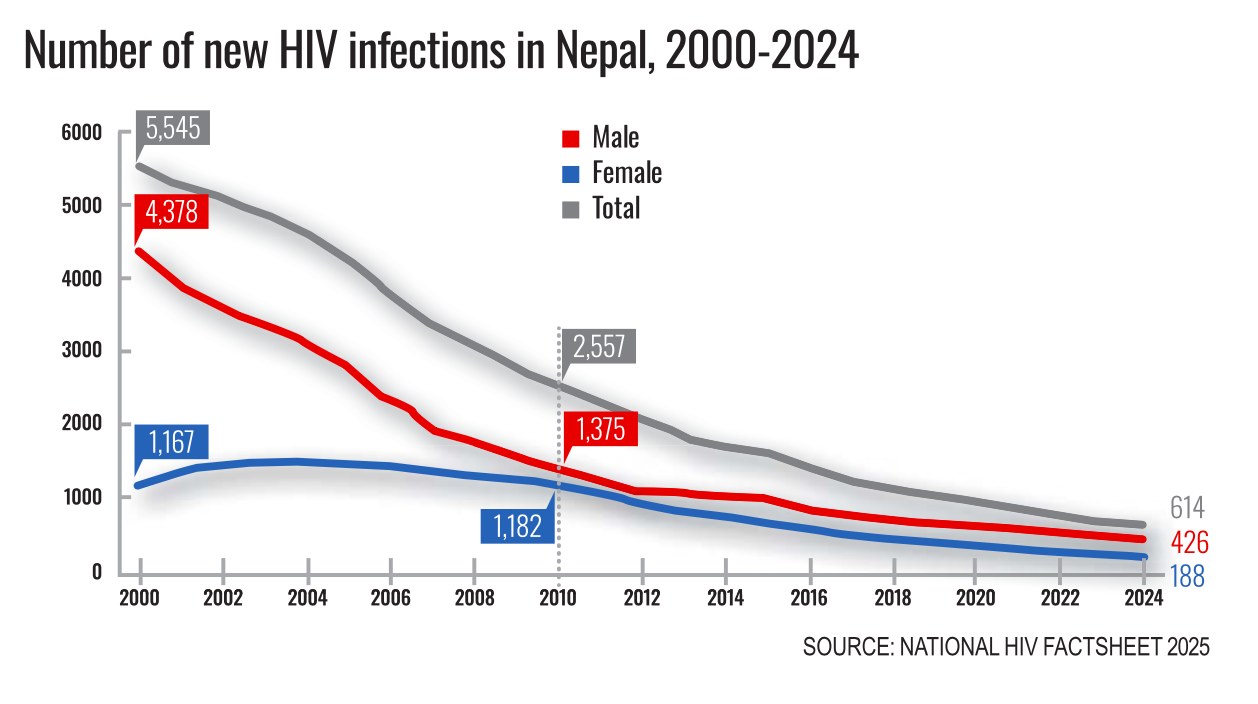
HIV/AIDS peaked in Nepal in the 1990s, spread through injecting drug use, unprotected sex, and from workers returning from India. Since then, the disease was largely under control because of the availability of antiretroviral therapy (ART). Annual reported cases dropped from 6,000 to a little over 600 in 2024.
However, there has been no drop in the social stigma associated with the infection. For people living with HIV across Nepal, disclosure of status is often the beginning of social and economic ostracisation.
However, with the pullout of USAID that was supplying ART to Nepal, there has been a recent resurgence. Most are in the 25-50 age group, and new diagnoses is mostly among women.
Parmita Ale, 43, had worked for years at a school canteen in Gorkha until her HIV status was disclosed to her employers six years ago without her consent. What followed was collective exclusion after a community meeting convened to terminate her.
“They pressured me to sign a resignation letter,” she recalls. “I told them I wouldn’t sign. I had been cooking and serving there for over a decade without anyone getting sick.”
But she was eventually fired. Ale relied on her Rs10,000 monthly salary to raise three children, and she has now gone back to subsistence farming.
Ramesh Rai received his HIV diagnosis last November during mandatory medical screening before leaving for Romania. “The manpower agency told me over the phone about the diagnosis, and all my plans went up in smoke,” he told us.
Ramesh is now a daily wage labourer at a garage in Itahari, barely earning enough to pay for food and rent. He has not told his family yet. “It is a huge burden to keep this a secret,” he said, breaking down. “I feel like my life has shattered like a mirror.”
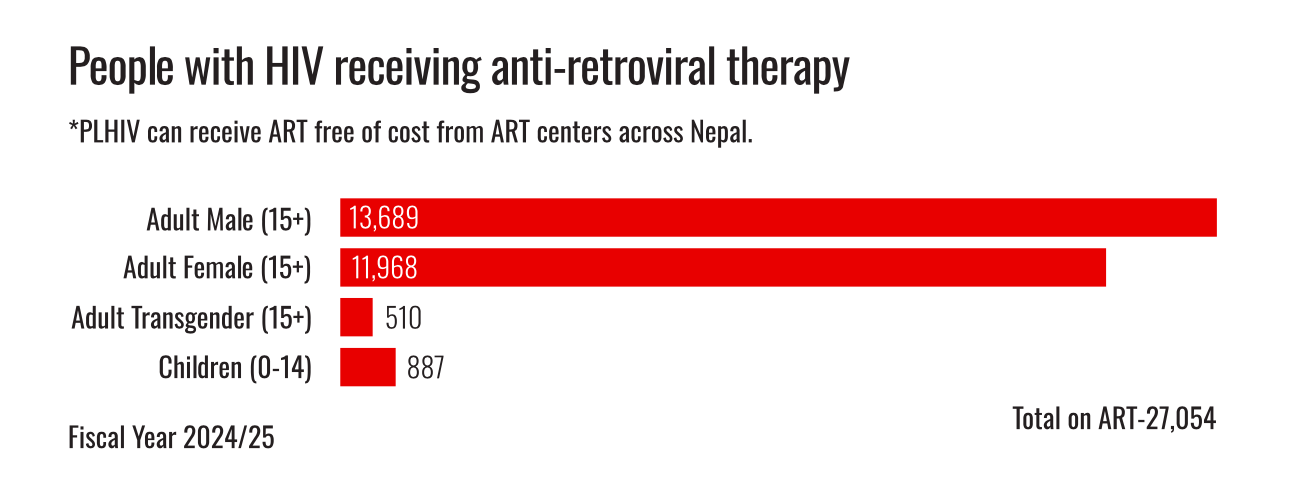
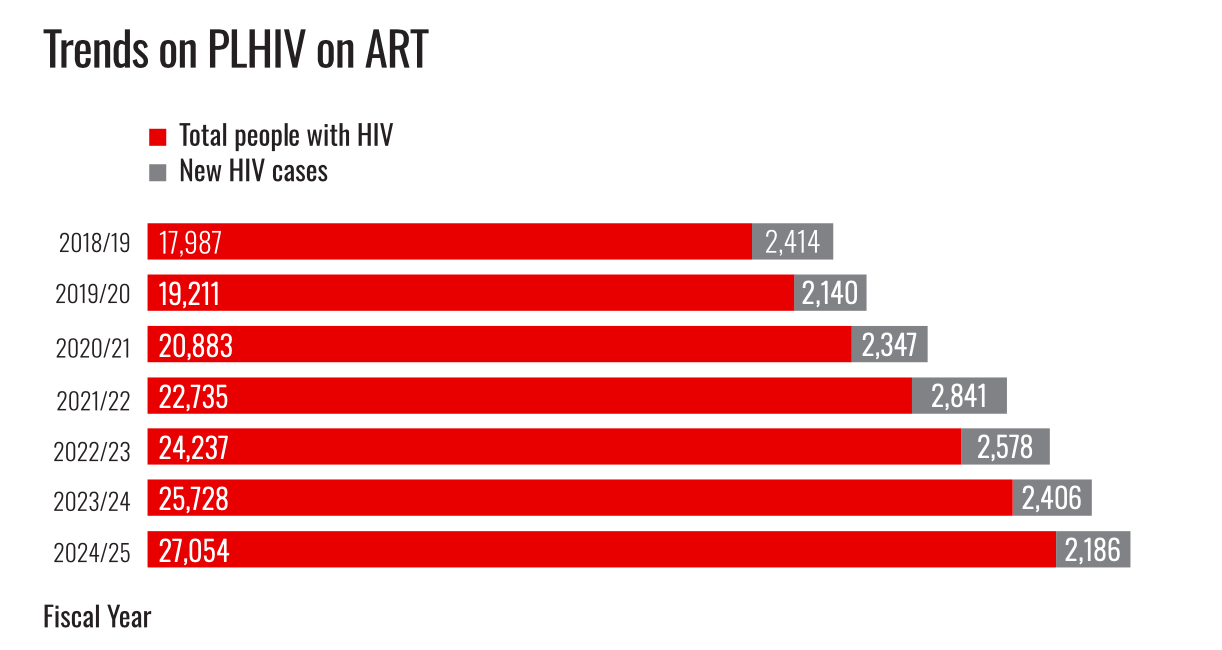
More than 27,000 people living with HIV are receiving treatment at the government’s 96 ART clinics across the country. About half of them got support from the AIDS Healthcare Foundation (AHF) Nepal, covering transportation costs, lab tests and nutrition support.
But more treatment centres and better support have not translated into social acceptance. A 2024 study by the National Human Rights Commission (NHRC) found that many people living with HIV are still denied employment, education, and even citizenship.
The People Living with HIV Stigma Index 2.0 Nepal, 2022 survey showed that while overt discrimination has declined from 49.7% in 2011 to 9.5% in 2022, hidden stigma remains pervasive.
In a survey of 927 respondents across 21 districts, more than half reported hiding their status, while only 17% had disclosed their diagnosis to employers. Of those whose status was known to their colleagues, 22% said the disclosure had occurred without their consent.
Explains Manju Adhikari of Teku ART Centre: “The science is not the problem. The medicine works, the real problem is the failure to remove the social stigma.”
The National Integrated Biological Behavioural Surveillance among Male Labour Migrants which surveyed 1,873 people across 14 districts in 2024 showed that 41.3% of respondents believed that a person living with HIV who is not yet sick should not be allowed to continue working.
One in two migrants said they would refuse to buy goods from a shopkeeper known to have HIV.
Adhikari provides psycho-social counselling to people living with HIV, and has witnessed the quiet epidemic of workplace expulsions. She remembers a construction labourer who disclosed his HIV status to co-workers. Soon after, his employer asked him to leave, claiming he was “unable to work”.
Experts say migration is common among people living with HIV. Due to stigma and discrimination, many are distanced from family and hometowns, losing support systems, livelihoods, and agency.
“Many people initially go to private clinics that charge Rs7,000 to Rs10,000 for baseline tests that cost only Rs1,700 to Rs1,800 at an ART Centre,” Adhikari says.
LEGAL VACUUM
Nepal’s Constitution as well as its Public Health Act 2018 prohibits discrimination based on a person’s health status, and the 2017 Labour Act requires due process for termination of employment.
The ILO Code of Practice on HIV/AIDS (1998) even encourages employers to provide special measures such as assigning staff lighter duties or more suitable work, instead of firing them if their job is physically demanding. But such legislation is limited to paper. People living with HIV can file legal cases under pseudonyms to protect their identity and avoid social stigma following the Supreme Court’s 2007 Confidentiality Guideline. However, many are unaware of this provision.
Workers seeking reinstatement can also file a case within 35 days of receiving notice of termination. But experts and activists say this short window is often impossible to meet for individuals dealing with stigma, emotional distress, and sudden loss of income. Which is why, despite protection, very few people living with HIV pursue legal action. Most isolate themselves from society to avoid the risk of wider disclosure and discrimination.
Bibek Yadav, spokesperson for the Department of Labour and Occupational Safety, confirms that not a single case related to HIV-based dismissal has formally reached the labour courts so far. The long process exhausts victims, and many give up when justice is not immediate, or eventually drop their cases. While the NHRC identifies issues of people living with HIV, it can only direct its recommendations to the relevant bodies.
A 2015 legal assessment of Nepal's HIV response policy led by NCASC found that the National Policy on HIV/AIDS in the Workplace (2007), which prohibits mandatory HIV testing, is poorly implemented.
The Nepal Police, Armed Police Force, and Nepal Army, continue to conduct mandatory HIV screenings during recruitment. Candidates who test positive are disqualified. A 2024 directive from the Ministry of Labour mandates HIV I and II tests for all foreign employment, regardless of destination, and allows physicians to order frequent testing for ‘risk groups’.
The long-pending HIV Bill, which activists and experts have advocated since 2009, remains stalled. Nabin Aryal, 50, who has been living with HIV and was ousted from his teaching job 20 years ago, is still desperately waiting for the Bill to fight his long-overdue and humiliating expulsion.
He says, “I have not returned to my village since then. I migrated to Kathmandu. I worked as a paper boy for years. “I underwent surgery for a brain tumour, and am vulnerable to opportunistic diseases.”
Lok Bahadur Lopchan, Under Secretary and Grievance Hearing Officer at the Ministry of Education and Sports, says that cases of discrimination faced in schools by employees must be reported to local authorities. But in reality no such complaints reach formal grievance mechanisms.
For people living with HIV across Nepal, legal provisions meant to protect them remain out of reach, and figuring out how to pay rent as putting food on the table for their families takes precedence.
Names and identifying details have been changed.