

Central Africa may seem too far away for most Nepalis to worry about the spread of Ebola, but the presence of Nepali UN peacekeepers at the epicenter of the epidemic has raised concern.
The Nepali Army has mandated a 21-day quarantine for any of its soldiers returning from peacekeeping duties in the Democratic Republic of Congo (DRC). Infectious disease experts say the country should remain on high alert, but not panic.
“The increased movement of people means we have to be prepared for any infection in any part of the world as we have previously with swine flu, Mpox, or the Omicron variant of Covid,” says virologist Sher Bahadur Pun at Teku Hospital. “An average of six Nepalis take yellow fever vaccines every day in our hospital, which proves that Nepalis are increasingly travelling to sub-Saharan Africa.”
There are 960 Nepali peacekeepers with MONUSCO (UN Organisation Stabilization Mission) and they are stationed in and around Bunia of Ituri province which is at the epicentre of the current outbreak which has seen the fastest yet spread of the rare Bundibugyo strain. Two suspected cases in Brazil and Italy tested negative.
Over 1,000 people have been infected and 250 have died in the DRC and neighbouring Uganda, and the World Health Organization (WHO) declared a Public Health Emergency of International Concern. The fatality rate of this strain named after a town in Uganda is between 30-50%. Victim's body remains highly contagious even days after death.
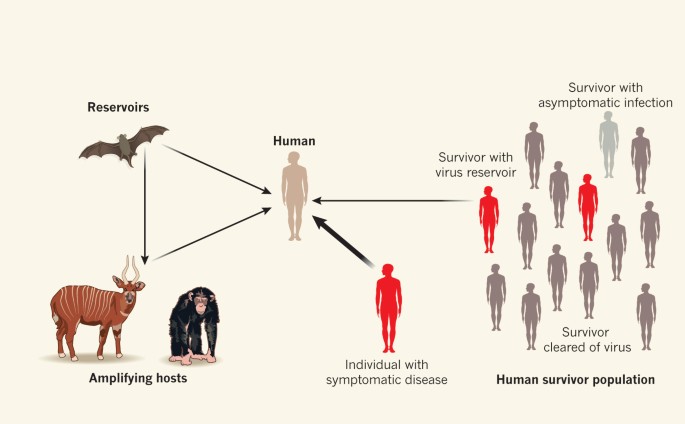
First detected in South Sudan in 1976, Ebola hemorrhagic fever is spread by fruit bats and human-to-human transmission happens through direct contact with the bodily fluids of an infected person. The virus has an incubation period of up to 21 days and symptoms develop within 8-10 days starting with fever, headache, muscle pain, fatigue and sore throat, before it gets more serious.
This means Nepal needs well-equipped and strict quarantine and isolation centres with trained staff not just for Ebola but for other future epidemics. Given Ebola’s high fatality rate and stigma, health officials say the government needs to revive the quarantine centres it had for Covid in 2020. However, some of those shelters in Kathmandu now house the landless evicted from squatter settlements last month.
“In many ways, Covid served as good training for us to prepare for other new and emerging infections,” says infectious diseases specialist Anup Subedee. “We have learnt some of the lessons but the same cannot be said institutionally. We still have last-minute mindset and wait until it is too late. We have to prepare, not panic.”
What makes the current Ebola outbreak even more challenging is the lack of resources on the ground where health workers were handling the patients only with surgical masks. Several doctors and health workers in Congo have already died from the infection they were treating their patients for.
PULLOUT FALLOUT
The USAID’s financial and technical support in rural and conflict torn areas like DRC was crucial in containing previous outbreaks of Ebola, each time with robust surveillance as well as timely testing and contact tracing to prevent further spread of the virus. This is the 17th outbreak of the virus in the DRC, but this time the rapid spread of the virus is a fallout of the USAID pullout.
“The outbreak this time is pretty serious, and it was spreading for a month and a half before it was detected, and even now only one-fourth of the required contact tracing is being done,” says Subedee. “Much of this has to do with the United States pulling out from WHO and the lack of USAID support for surveillance and containing the spread.”
Another reason for the rapid spread of the Ebola virus is that its symptoms are similar to malaria, cholera, typhoid and other viral hemorrhagic fevers, so that when infected patients are admitted to hospitals they spread it to non-infected patients. It also takes days for results of sample tests to be confirmed during which time there is more mingling of patients.
Just like with Covid, health authorities in Nepal have to be especially alert to the mesures being taken in India with which the country shares an open border. India has already issued a travel advisory urging citizens to avoid non-essential travel to the DRC, Uganda and South Sudan. The Indian government even postponed its fourth India-Africa Forum Summit, which was to be held in Delhi from 28-31 May.
Several other countries including the United States, Canada, the UAE and Thailand have issued travel advisories and border restrictions for the DRC, Uganda and South Sudan following the spread of the Bundibugyo strain.
Africa accounts for less than 1% of visitors to Nepal and most of them are from Egypt, Morocco and South Africa. Even so, Kathmandu airport and all the border checkpoints have been alerted for arrivals from central Africa.
“We need heightened surveillance, especially along the Indian border. We have to prevent Ebola from entering Nepal because no hospital here is equipped to handle it,” warns Pun. “By designation our Infectious Diseases Hospital in Teku is the only one that can take in Ebola patients but it will soon overwhelm us if precautions are not taken. The government must think urgently about upgrading existing facilities and make healthcare a priority.”
Bird flu alert
Bird flu alerts have become so common in Nepal that the public tends to ignore them. Health officials say that although the threats so far are low, people need to be vigilant.
The recent detection of highly pathogenic avian influenza in poultry farms in three wards on the northern outskirts of Kathmandu has raised health concerns. All poultry, along with eggs and feed, in the affected areas were destroyed.
Nepal is on the Central Asian Flyway for migratory birds that make roundtrips across the Himalaya every year, and Kathmandu Valley’s wetlands are popular stopover for the wintering birds. One such spot is Taudaha Lake, and 15 birds were found dead there in March. Crows and other urban birds are also dying near the Teaching Hosptial and Patan.

Aquatic birds are the primary reservoirs of the virus, and it can cause mild to severe illness when it spills over into domestic poultry and even mammals. Human-to-human transmission is rare, but the danger is infection is high among poultry workers. Because the virus does not survive at 70°C or above, meat and egg consumption is safe when properly cooked.
“Poultry farmers, those who transport and handle them as well as slaughter houses are at high risk since they are in contact with secretion, faces and feathers,” says Sher Bahadur Pun, virologist at Infectious Disease Hospital in Teku. “We have to pay close attention to signs of spreading, there have been human fatilities in the past.”
Pun says his hospital has treats three patients recently with mild symptoms, but that there may be more unreported cases. “But viruses are always mutating and they might become more virulent, especially when they jump the species barrier,” he adds.
Vaccines against bird flu are not readily available in Nepal, although the United States and Canada have strategic stockpiles against the H5N1 strain for high-risk populations. As for treatment, the prescription antiviral oseltamivir (Tamiflu) used for influenza, has been found to be most effective for bird flu patients.
Sonia Awale